CASE OF A 60/M CVA WITH RIGHT SIDED HEMIPARESIS 2° TO HYPERTENSIVE BLEED
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE :
A 60 year old man, carpenter by occupation came to the casuality with
CHIEF COMPLAINTS
Loss of speech since morning
HISTORY OF PRESENT ILLNESS :
Patient was apparently asymptomatic 3 years ago
3 years back, where he attended a family function and had an binge of alcohol consumption, after a few hrs of consumption, he suddenly developed deviation of angle of mouth towards left side, for which the attenders took him to a local hospital .He was treated conservatively (? Medication unknown) and adviced to use those medications for 1 week.After a week ,his deviation of mouth was resolved.There in the hospital he was diagnosed of having a renal problem ,as B/L pedal edma (pitting type) extending up to knee and facial puffiness was found to be present on examination.He was diagnosed of having HTN and was adviced to use antihypertensives.His creatinine & blood urea were found to be elevated .He was given lasixs and sodium bicarbonate (OD). From then he used to have similar episodes of B/L pedal edema (3-4 episodes till now) and facial puffiness which used to get resolved after using medications since 3 years.Since then he quitted his daily routine work and was restricted to home.
Similar episode occured after 1 year with weakness of right upper and lower limb along with deviation of angle of mouth towards left.He again was taken to a local hospital where conservative management was done .He was adviced to use those medications ( Ecospirin, atorvastatin and clopidogrel ) and daily physiotherapy exercises of right UL and LL .He stayed there for 10 days and got discharged.since then patient started using walking aids.
6 months back he had complaints of pain in the neck and around occipital region ,for which they went to hospital and medications were given (? NSAIDS). pain subsided in 5 days
Yesterday night after having dinner, 30 mins later he complained of having pain in throat and went to sleep.Today morning while he woke up he lost his speech and was unresponsive.He is conscious and oriented to time ,place and person during the episode.In view of this,he was taken to hospital where his BP was found be 220/120 (medication given) and a MDCT brain was done showing 26 x 56 mm acute hemorrhage in the right lentiform nucleus.He was then referred to kims
TIMELINE OF EVENTS

PAST HISTORY :
He was a k/c/o Type 2 DM 5 years back (diagnosed on routine health check up)
and HTN since 3 years and was on regular medication since then
HTN (Tab Clinidipine 10 mg,tab metoprolol and tab clonidine )
DM2 ( tab gliclazide 40 mg OD)
K/C/O CVA (3 yrs back)
5 years back he was operated for ? lipoma (over the back of left scapular region)
Not a k/c/o TB,CAD, Asthama ,thyroid and epilesy
PERSONAL HISTORY :
Mixed diet
Sleep adequate
Appetite normal
Bowel and bladder movements regular
He was a known alcoholic since 30 years.Drinks regularly 90 ml whisky.Quitted drinking 3 years back
VITALS :
GCS : E4V1M5
Temp: Afebrile
PR: 88 bpm
BP: 200/100 mm hg
RR: 14 cpm
Spo2 - 98% at RA
GRBS - 150 mg/dl
GENERAL EXAMINATION :
Patient is conscious, coherent and cooperative
Moderately built and moderately nourished
PALLOR +
No icterus,clubbing,cyanosis,koilonychia, edema and lymphadenopathy



SYSTEMIC EXAMINATION
CVS :
Inspection:
Chest wall is bilaterally symmetrical.
No precordial bulge
Palpation:
JVP - normal
Apex beat - felt in the left 5th intercostal space in the mid clavicular line.
Auscultation:
S1, S2 heard , No murmurs
RS :
Position of trachea: central
Bilateral air entry +
NVBS heard
PER ABDOMEN :
Soft, non distended and non tender
No organomegaly
Bowel sounds heard
No palpable mass or fluid present
CNS :
Patient is Conscious
1. Higher mental functions
a) Appearance & behaviour - moderately built , oriented to time,place and person
b) Level of consciousness - conscious
c) Speech & language - No response
c) Cognitive functions - oriented to time,place and person
- MMSE : not elicited
2. Cranial nerves
1. Olfactory : Not elicited
2. Optic : visual acuity,Visual field,colour vision,reflexes : not elicited
3. Occulomotor, trochlear & abducent :
Pupils are reactive and normal
No ptosis & nystagmus
4. Trigeminal :
Sensory - not elicited
Motor - not elicited
Corneal reflex - present
Conjuctival reflex - present
7. Facial nerve :
Motor: nasolabial folds present on both sides,
deviation of angle of mouth to the left side
Sensory: taste not elicited
Secretomotor moistness of eye and tongue normal, buccal mucosa normal
8. Vestibulocochlear - Rinnes & weber not elicited
9. Glossopharyngeal & Vagus : Gag not elicited, uvula was centrally placed
11. Spinal accessory :
Trapezieus not elicited
Sternocleidomastoid not elicited
12. Hypoglossal : no deviation of tongue, no wasting, no fibrillations
3.Motor system :
- Attitude & position : patient in supine position with right lower leg externally rotated
- Bulk : normal , no wasting
- TONE:
Rt Lt
UL N N
LL hypertonia hypertonia
- POWER:
Rt Lt
UL 4/5 4/5
LL 3+/5 +3/5
- REFLEXES :
•Superficial Rt Lt
Corneal : +2 +2
Conjunctival : +2 +2
Abdominal : +2 +2
• Deep Rt Lt
Biceps : +3 +2
Triceps : +3 +2
Supinator : + Absent
Knee jerk : +3 +3
Ankle jerk : +3 +3
Plantar : flexor flexor
4. Sensory system -
Superficial -fine touch,temperature,pain -present over all the four limbs
Deep-position ,vibration,crude touch,stereognosis, 2 point discrimination - present
5. Cerebellum
Titubation - absent
Nystagmus- absent
Intentional tremors - absent
Pendular knee jerk - absent
Coordination tests :
Finger nose test - present
Finger finger test - incoordination
Knee heel test - present
Romberg test - not elicited
Gait - not elicited
6. No meningeal signs
INVESTIGATIONS :
4/09/21 (outside the hsptl)
Hemogram
Hb: 9.4 gm/dL
TLC: 11,500 cells/cu mm
Neutrophils: 73%%
Lymphocytes: 19 %
Eosinophils - 6%
Monocytes - 2%
Basophils - 0%
PCV - 28.2 vol %
RBC: 3.1 millions/cu mm
Platelets: 1.95 lakh cells/cu mm
RFT :
Serum creatinine: 6.9 mg/dl
Urea - 98.4 mg/dl
Serum uric acid - 12
Sr.calcium - 8.0 mg/dl
Sodium - 131 meq/l
K+ - 3.4 meq/l
Cl- 97 meq/l
RBS - 139 mg/dl
MDCT SCAN OF BRAIN (plain)
- 26 x 15 mm acute hemorrhage in right lentiform nucleus
- Features suggestive of hypertensive hemorrhage
- Old infarcts in left lentiform nucleus and corona radiata

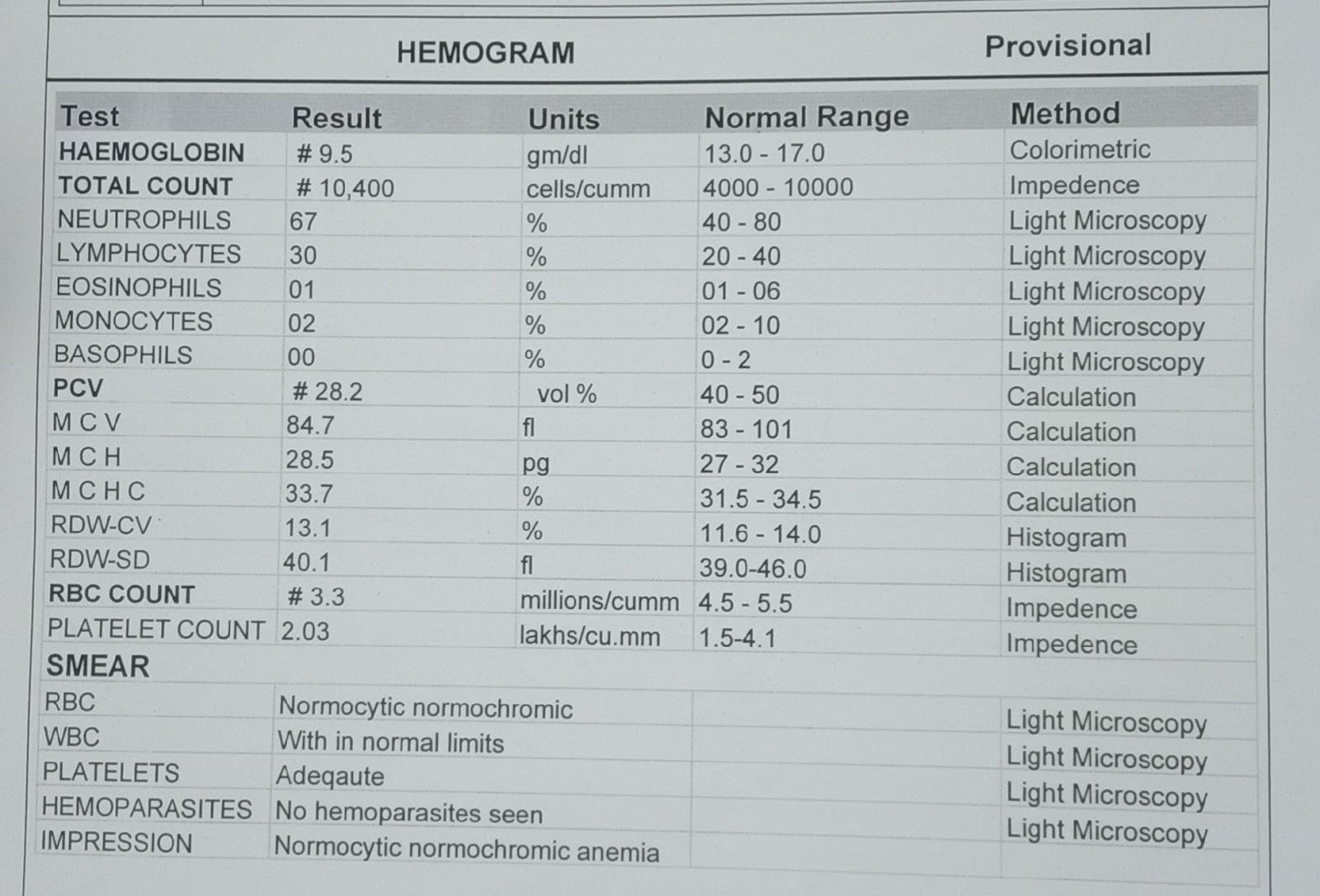
5/09/2021
Hemogram :
Hb: 9.5 gm/dL
TLC: 10,400 cells/cu mm
Neutrophils: 67%
Lymphocytes: 30 %
PCV - 24.2 vol %
MCV - 84.7 fl
MCHC - 33.7%
MCH - 28.5 pg
RBC: 3.3 millions/cu mm
Platelets: 2.03 lakh cells/cu mm
CUE :
Albumin: ++
Sugars: nil
PC: 3-6
EC: 2-3
RBC: nil

RFT :
Serum creatinine: 6.6 mg/dl
Urea - 142 mg/dl
Sodium - 139 meq/l
K+ - 4.1 meq/l
Cl- 105 meq/l



LFT :
Total bilirubin: 1.03 mg/dl
Direct bilirubin: 0.23 mg/dl
SGOT: 10 IU/l
SGPT: 10 IU/l
ALP: 162 IU/l
Total protein: 5.9 gm/dl
Albumin: 3.3 gm/dl
A/G: 1.30

RBS - 107 mg/dl
FBS - 105 mg/dl
HBA1C - 6.4%
PPBS - 81 mg /dl




CXR-PA view

ECG




Serum creatinine

7/09/21
USG abdomen & pelvis






PROVISIONAL DIAGNOSIS :
CVA with right sided hemiparesis secondary to hypertensive bleed
With ? CKD
K/C/O type 2 DM since 5 years & HTN since 3 years
BP TRENDS

FEVER CHARTING

TREATMENT :
DAY O
Ryles tybe inserted
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj pantop 40 mg IV/OD
3. Inj optineuron 1 amp in 100 ml NS slow IV/OD
4. Inj zofer iv/sos
5. Inj mannitol 100ml /IV/TID
6. Tab clinidipine 10 mg PO/BD
7. Inj HAI s/c TID
( 8am...4pm...8pm)
8. GRBS charting 4th hourly
9. B.P/PR/Temp monitoring 4th hourly
10. I/O charting
DAY 1
Vitals :
Afebrile
Bp- 200/100 mm hg
PR - 94 bpm
RR - 15 cpm
SPO2-97% at RA
GRBS - 148 mg/dl
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2.Inj optineuron 1 amp in 100 ml NS slow IV/OD
3. Inj mannitol 100ml /IV/TID
4.Tab clinidipine 10 mg PO/BD
5.Tab Arkamin 0.1 mg PO/TID
6.Tab Prazosin 5 mg PO/BD
7.Tab MET-XL 50 mg PO/OD
8.Tab Levipil 500 mg PO/BD
9.Tab pan 40 mg Po/OD
10.Inj HAI s/c TID
( 8am...4pm...8pmm..2am)
11. GRBS charting 6th hourly
12. B.P onitoring 4th hourly
13. I/O charting
14. Tab Nodosis 500 mg PO/BD
15. Physiotherapy of right UL and LL
DAY 2
SOAP NOTES :
SUBJECTIVE
Slurring of speech +
New complaint:
Pain in the left loin
OBJECTIVE
Temperature : Afebrile
Bp- 150/80 mm hg
PR - 90 bpm
RR - 15 cpm
SPO2- 98% at RA
GRBS - 97 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O type 2 DM since 5 years & HTN since 3 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3. Inj mannitol 100ml /IV/TID
4.Tab clinidipine 10 mg PO/BD
5.Tab Arkamin 0.1 mg PO/TID
6.Tab Prazosin 5 mg PO/BD
7.Tab MET-XL 50 mg PO/OD
8.Tab pan 40 mg Po/OD
9.Inj HAI s/c TID
( 8am...4pm...8pmm..2am)
10. GRBS charting 6th hourly
11. B.P onitoring 4th hourly
12. I/O charting
13. Tab Nodosis 500 mg PO/BD
14. Physiotherapy of right UL and LL
DAY 3
SOAP NOTES :
SUBJECTIVE
Slurring of speech +
New complaint:
Pain in the left loin
OBJECTIVE
Temperature : Afebrile
Bp- 140/80 mm hg
PR - 88 bpm
RR - 15 cpm
SPO2- 98% at RA
GRBS - 100 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O CVA & DM2 since 5 years & HTN since 3 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3. Inj mannitol 100ml /IV/BD
4.Tab clinidipine 10 mg PO/BD
5.Tab Arkamin 0.1 mg PO/TID
6.Tab Prazosin 5 mg PO/BD
7.Tab MET-XL 50 mg PO/OD
8.Tab pan 40 mg Po/OD
9.Inj HAI s/c TID
( 8am...4pm...8pmm..2am)
10. GRBS charting 6th hourly
11. B.P onitoring 4th hourly
12. I/O charting
13. Tab Nodosis 500 mg PO/BD
14. Physiotherapy of right UL and LL
DAY 4
SOAP NOTES :
SUBJECTIVE
Slurring of speech +
Left loin pain decreased
OBJECTIVE
Temperature : Afebrile
Bp - 150/100 mm hg
PR - 82 bpm
RR - 16 cpm
SPO2- 98% at RA
GRBS - 72 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O CVA & DM2 since 5 years & HTN since 3 years
Chronic alcoholic since 30 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3.Tab clinidipine 10 mg PO/BD
1 -----x----- 1
4.Tab Arkamin 0.1 mg PO/TID
1 -----1 ----- 1
5.Tab Prazosin 5 mg PO/BD
1 .....x..... 1
6.Tab MET-XL 50 mg PO/OD
x --- 2pm ---x
7.Tab pan 40 mg Po/OD
8.Inj HAI s/c TID
( 8am...4pm...8pm..2am)
9.Tab ultracet 1/2 tab QID
10. GRBS charting 6th hourly
11. B.P monitoring 4th hourly
12. I/O charting
13.Physiotherapy of right UL&LL
Slurring of speech +
Left loin pain decreased
OBJECTIVE
Temperature : Afebrile
Bp - 150/100 mm hg
PR - 82 bpm
RR - 16 cpm
SPO2- 98% at RA
GRBS - 72 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O CVA & DM2 since 5 years & HTN since 3 years
Chronic alcoholic since 30 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3.Tab clinidipine 10 mg PO/BD
1 -----x----- 1
4.Tab Arkamin 0.1 mg PO/TID
1 -----1 ----- 1
5.Tab Prazosin 5 mg PO/BD
1 .....x..... 1
6.Tab MET-XL 50 mg PO/OD
x --- 2pm ---x
7.Tab pan 40 mg Po/OD
8.Inj HAI s/c TID
( 8am...4pm...8pm..2am)
9.Tab ultracet 1/2 tab QID
10. GRBS charting 6th hourly
11. B.P monitoring 4th hourly
12. I/O charting
13.Physiotherapy of right UL&LL
DAY 5
SOAP NOTES :
SUBJECTIVE
Slurring of speech +
Left loin pain (resolved)
OBJECTIVE
Temperature : Afebrile
Bp - 150/90 mm hg
PR - 84 bpm
RR - 16 cpm
SPO2- 98% at RA
GRBS - 81 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O CVA & DM2 since 5 years & HTN since 3 years
Chronic alcoholic since 30 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3.Tab clinidipine 10 mg PO/BD
1 -----x----- 1
4.Tab Arkamin 0.1 mg PO/OD
1 -----x ----- x
5.Tab MET-XL 50 mg PO/OD
x --- 2pm ---x
6.Tab lasix 40 Mg PO/BD
7.Tab pan 40 mg PO/OD
8.Inj HAI s/c TID
( 8am...4pm...8pm..2am)
9.Tab ultracet 1/2 tab QID
10. GRBS charting 6th hourly
11. B.P monitoring 4th hourly
12. I/O charting
13. Physiotherapy of right UL and LL
SUBJECTIVE
Slurring of speech +
Left loin pain (resolved)
OBJECTIVE
Temperature : Afebrile
Bp - 150/90 mm hg
PR - 84 bpm
RR - 16 cpm
SPO2- 98% at RA
GRBS - 81 mg/dl
ASSESSMENT:
CVA with right sided hemiparesis secondary to hypertensive bleed
? CKD
K/C/O CVA & DM2 since 5 years & HTN since 3 years
Chronic alcoholic since 30 years
PLAN OF CARE:
1.RT feeds
100 ml plain water 1 hourly
200 ml milk with protein powder 2nd hourly
2. Inj optineuron 1 amp in 100 ml NS slow IV/OD
3.Tab clinidipine 10 mg PO/BD
1 -----x----- 1
4.Tab Arkamin 0.1 mg PO/OD
1 -----x ----- x
5.Tab MET-XL 50 mg PO/OD
x --- 2pm ---x
6.Tab lasix 40 Mg PO/BD
7.Tab pan 40 mg PO/OD
8.Inj HAI s/c TID
( 8am...4pm...8pm..2am)
9.Tab ultracet 1/2 tab QID
10. GRBS charting 6th hourly
11. B.P monitoring 4th hourly
12. I/O charting
13. Physiotherapy of right UL and LL

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment